.svg)
How the Gut Microbiome Shapes Human Longevity: A Clinically Grounded, High-Impact Overview

In longevity medicine, we often emphasize genetics, cellular repair pathways, and mitochondrial function. However, one of the most powerful and modifiable drivers of healthy aging resides within the gastrointestinal tract: the gut microbiome. This complex ecosystem of bacteria, archaea, fungi, and bioactive metabolites functions as a central control hub for inflammation, metabolic health, cognitive performance, immune resilience, and overall lifespan.
Cutting-edge research—including genomics, multi-omics profiling, and Mendelian randomization studies—now shows that specific gut microbial patterns are not just associated with longer life; they play a causal role in longevity. By understanding how these microbes influence aging biology, we can move beyond generic wellness guidance and implement evidence-based, precision strategies that support optimal gut health, slow biological aging, and promote long-term vitality.
Executive Summary
- Your gut microbiome is a key driver of how you age, influencing inflammation, metabolism, immunity, and cellular energy—and it’s one of the most modifiable systems in the body.
- Healthy aging depends on the right microbes doing the right jobs, not just “more diversity.” Beneficial bacteria support gut integrity and metabolic health, while harmful patterns accelerate aging.
- Science now shows this relationship is causal, meaning the microbiome doesn’t just reflect health—it actively shapes longevity.
- Targeted, data-driven gut strategies can meaningfully improve healthspan, moving beyond generic diet advice to personalized interventions that slow biological aging.
The Microbiome as a Biological Regulator of Healthy Aging
Diversity: A Holistic but Context-Dependent Marker
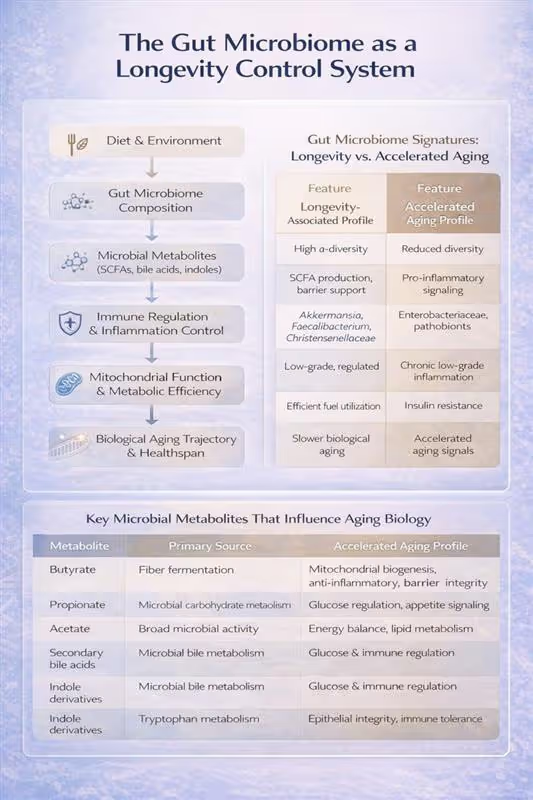
In most populations, greater microbial diversity corresponds to metabolic flexibility, reduced inflammation, and youthful immune function. Centenarians commonly exhibit higher overall diversity.
However, at least one large study of genetically long-lived individuals reported lower microbial diversity, implying that diversity is beneficial but not universally predictive. Composition and function may matter more than diversity alone.
Key Longevity-Associated Microbes
Large cohort studies and Mendelian randomization analyses consistently highlight several organisms linked to improved lifespan:
Positively associated with longevity
- Akkermansia muciniphila
- Alistipes species (e.g., A. senegalensis, A. shahii)
- Subdoligranulum
- Enrichment in centenarians: Eisenbergiella tayi, Methanobrevibacter smithii, Hungatella hathewayi, Desulfovibrio fairfieldensis
Negatively associated with longevity
- Fusobacterium nucleatum
- Bacteroides massiliensis
- Certain Streptococcus species
These patterns are reproducible across multiple aging cohorts, suggesting the microbiome is not just a bystander but a driver of longevity biology.
How the Microbiome Influences Aging
Several biological pathways explain how gut microbes can accelerate or slow aging:
- Short-chain fatty acid (SCFA) production
SCFAs—especially butyrate—strengthen the gut barrier, reduce inflammation, support metabolic health, and regulate immune function. Long-lived individuals show enhanced SCFA-producing pathways.
- Secondary bile acid metabolism
Beneficial bacteria help maintain bile-acid balance, which influences cholesterol metabolism, glucose homeostasis, and cellular stress responses.
- Purine recycling & vitamin K2 production
These processes support mitochondrial efficiency, cardiovascular health, and prevention of age-related disease.
- Gut-immune, gut-brain & gut-muscle axes
The microbiome modulates systemic inflammation, immune aging (immunosenescence), cognitive health, and muscle function—all central pillars of healthy aging.
Experimental Evidence: Causality, Not Just Correlation
Animal Models
- Transplantation of healthy wild-type microbiota into progeroid mice extended both healthspan and lifespan.
- Akkermansia muciniphila alone was sufficient to improve gut barrier integrity, reduce inflammation, and promote longevity.
- In C. elegans, A. muciniphila administration extended lifespan, highlighting conserve cross-species effects.
Dr. Banerjee is a board-certified gastroenterologist with over 15 years of clinical experience, peer-reviewed publications indexed in PubMed, and deep expertise in gut microbiome science. He advises high-achieving individuals and families on precision longevity and healthspan optimization. Expanded clinical analysis is available through the Private Longevity Briefing.
Selected References
- Liu X, Zou L, Nie C, et al. Mendelian randomization analyses reveal causal links between the gut microbiome and longevity. Sci Rep. 2023;13:5127.
- Chen S, Chen W, Wang X, Liu S. Mendelian randomization supports causal relationships between gut microbes and lifespan. J Transl Med. 2024;22:1032.
- Zhang G, Lu Y, Wang Z, et al. Multi-omics MR study identifies causal gut microbiota–aging relationships. Arch Gerontol Geriatr. 2025;131:105765.
- Chen S, Zhang Z, Liu S, et al. Consistent microbiome signatures in long-lived human cohorts. Gut Microbes.2024;16:2393756.
- Araújo JR, Marques C, Rodrigues C, et al. Gut microbe–derived metabolites in aging and longevity. Ageing Res Rev. 2024;100:102451.
- Ai X, Liu Y, Shi J, et al. Structural characteristics of longevity-associated gut microbiota in China. Appl Microbiol Biotechnol. 2024;108:300.
- Bárcena C, Valdés-Mas R, Mayoral P, et al. Fecal microbiota transplantation extends lifespan in progeroid mice. Nat Med. 2019;25:1234–1242.
- Tseng CH, Wu CY. Review: microbiome dysbiosis and pathways to longevity. J Biomed Sci. 2025;32:93.
- Ling Z, Liu X, Cheng Y, et al. Gut microbiota and aging. Crit Rev Food Sci Nutr.2022;62:3509–3534.
Latest Articles
View all.jpg)
The Biological Cost of the Three-Home Life: Microbiome Stability for the Philadelphia–Naples–Palm Beach Circuit
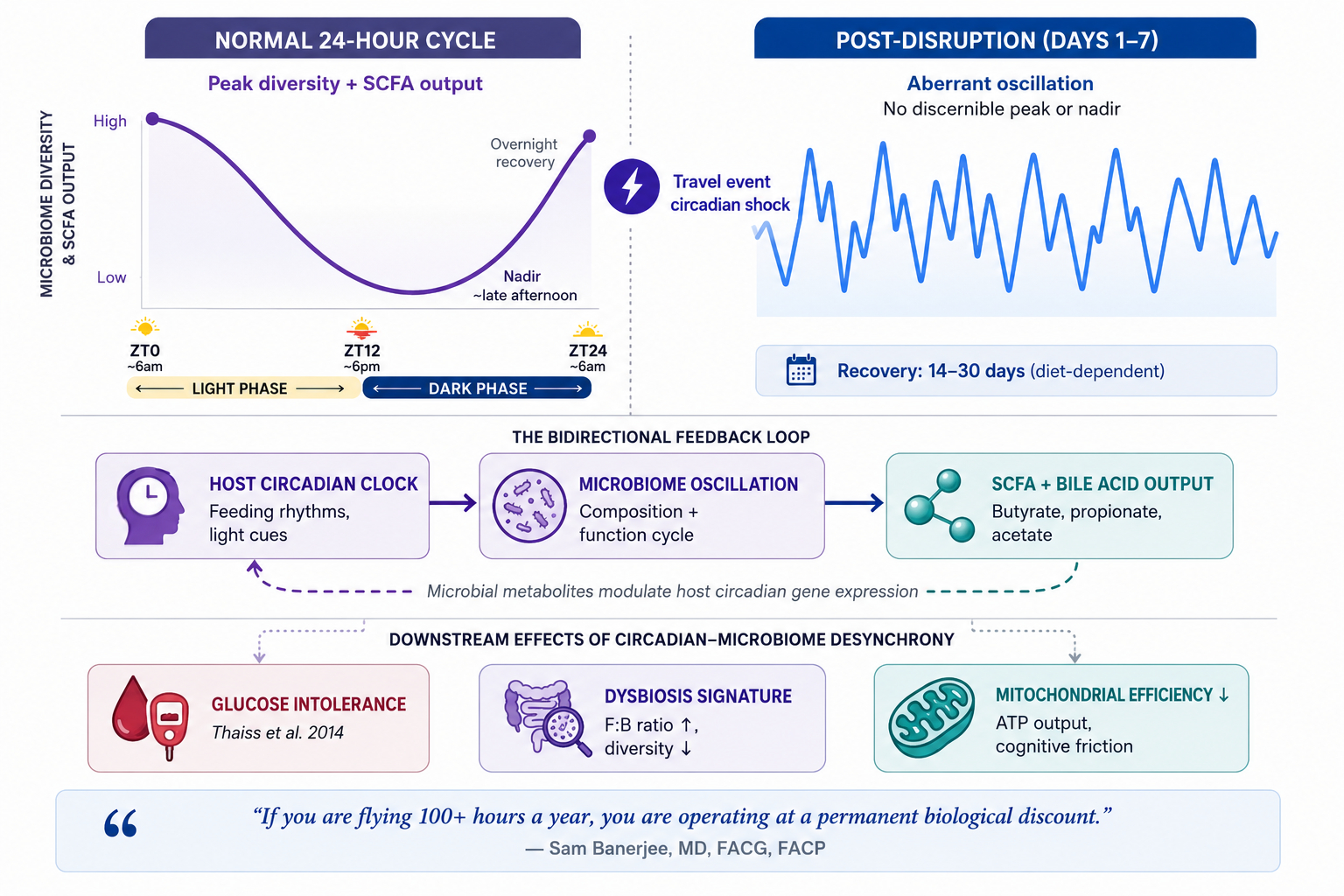
The most expensive part of your flight isn’t the fuel or the crew—it’s the initial 48-hour perturbation window your microbiome requires to begin stabilizing, the first phase of a recovery arc that, without intervention, runs 2–4 weeks. If you are flying 100+ hours a year across this circuit, you are operating at a permanent biological discount.
For the executive or family principal who splits the calendar between Philadelphia, Naples, and Palm Beach, that transition happens multiple times a year—sometimes monthly. The jet bridge, the climate shift, the change in diet and sleep schedule, the stress of compressed itineraries: each represents a perturbation event your gut ecosystem must absorb and recover from. When the frequency of those events outpaces the microbiome’s recovery window, the cumulative deficit shows up not as GI symptoms, but as accelerated inflammatory tone, metabolic drift, and cognitive friction that most high-performers quietly attribute to age or stress.
This is not a wellness concern. It is a biological capital concern. Understanding the mechanisms—and the specific variables the Philadelphia–Naples–Palm Beach circuit introduces—allows for targeted mitigation rather than generic advice about eating well and staying hydrated.
What Air Travel Actually Does to Your Gut
The popular narrative frames inflight microbiome disruption around cabin pressure and recycled air. The evidence points elsewhere. The three operative mechanisms are circadian disruption, dietary and environmental change, and—for frequent international travelers—acquisition of antimicrobial-resistant organisms. The Philadelphia–Naples–Palm Beach route is domestic, which limits the third risk, but the first two operate on every flight regardless of distance.
The circadian-microbiome feedback loop
Thaiss et al. demonstrated in a landmark 2014 paper that jet lag induces aberrant diurnal oscillations in gut microbiota composition—disruptions sufficient to promote glucose intolerance and obesity, with effects transferable to germ-free mice via fecal transplant. This is not a minor finding. It established that host circadian rhythm and microbiome composition are bidirectionally coupled: the microbiome oscillates in composition and function according to feeding rhythms, and when those rhythms are disrupted—as occurs with transmeridian travel—the ecosystem destabilizes.
Chronic circadian misalignment in murine models decreases microbial abundance, richness, and diversity; increases the Firmicutes-to-Bacteroidetes ratio (a recognized dysbiosis marker); and alters tryptophan and secondary bile acid metabolism. A 2025 systematic review confirmed these directional findings in humans, though diversity metrics remain variable across studies. The bidirectionality matters: microbial metabolites including short-chain fatty acids and bile acids modulate host circadian gene expression. Disrupt the host clock, and the microbiome destabilizes. Destabilize the microbiome, and the host clock’s resilience weakens. The feedback loop can self-perpetuate.
Dietary environment as a second perturbation axis
International travel literature provides the most granular data here. A metagenomic analysis of 267 US travelers found significant depletion of microbial diversity and enrichment of Enterobacteriaceae after travel, with 67% of subjects acquiring phylogenetically distinct new E. coli strains. Antibiotic resistance gene burden increased by a median of 15%. The Philadelphia–Naples–Palm Beach circuit does not expose the traveler to the pathogenic microbe profile of developing regions, but the dietary discontinuity—restaurant frequency, alcohol, altered meal timing, reduced prebiotic fiber intake—operates through identical mechanisms at a lower magnitude.
What Makes This Circuit Clinically Distinct
The Philadelphia–Naples–Palm Beach transition is not a single disruption event. For someone making this transition four to eight times annually across both Southwest Florida and the Palm Beach corridor, it is a recurring oscillation that the microbiome must absorb repeatedly, often without full recovery between cycles. Several variables compound the generic travel disruption:
Climate and dietary environment
Philadelphia and the Southwest Florida and Palm Beach corridor represent meaningfully different food environments. The Mediterranean-influenced dietary patterns more accessible in Philadelphia—high-quality olive oil, diverse vegetables, legume-forward eating—shift toward the restaurant-heavy, higher-alcohol, lower-fiber consumption patterns typical of seasonal life in Naples or Palm Beach. Every reduction in prebiotic fiber intake directly reduces SCFA production—particularly butyrate—which is the primary fuel for colonocytes and the upstream regulator of intestinal barrier integrity and systemic inflammatory tone.
Sleep architecture and schedule compression
The Philadelphia–Naples–Palm Beach transition is typically embedded in a compressed itinerary—departures timed around board meetings, closings, or social calendars. Sleep architecture disruption, even without transmeridian jet lag, is sufficient to shift the Firmicutes-to-Bacteroidetes ratio. A single night of poor sleep alters microbiome composition in ways measurable by morning. Over four to six transition events per year across both Florida markets, the cumulative effect on microbial diversity is not trivial.
The recovery window problem
A longitudinal study of travelers to the Caribbean found that gut microbial composition gradually shifted toward local enterotypes during extended stays, then reverted to original profiles within one month of returning home—mediated primarily by dietary normalization. The microbiome is resilient. But one month of recovery assumes the traveler stays home for a month. For the executive rotating quarterly across Philadelphia, Naples, and Palm Beach, the recovery window closes before the next transition opens.
The Gut–Mitochondria Axis: Why This Is an Executive Health Optimization Problem

Most travel health frameworks stop at the gut. The clinical picture extends further. The gut microbiome and mitochondrial function are bidirectionally coupled through a set of mechanisms that make travel-induced dysbiosis directly relevant to cognitive performance and metabolic output—not just digestive comfort.
Butyrate—the primary short-chain fatty acid produced by beneficial gut bacteria fermenting prebiotic fiber—stimulates mitochondrial biogenesis through PGC-1α activation and enhances oxidative phosphorylation efficiency. When butyrate-producing taxa are depleted by travel-associated dietary disruption and circadian desynchrony, the downstream consequence is measurably reduced mitochondrial ATP output. This is not a theoretical pathway. It is the mechanism by which gut dysbiosis translates into the cognitive friction and physical fatigue that frequent travelers normalize as the cost of doing business.
The second mechanism is barrier-mediated inflammation. Gut barrier failure—accelerated by the dietary shifts and circadian disruption of repeated travel—allows bacterial lipopolysaccharide to enter systemic circulation. The resulting inflammatory cytokine load directly reduces mitochondrial ATP efficiency and shifts cellular metabolism toward less efficient glycolytic pathways. Mitochondrial supplements including CoQ10 and NAD+ precursors demonstrate measurably reduced efficacy when gut dysbiosis persists—a finding with direct implications for the significant supplement expenditure common among health-conscious executives. You cannot optimize the downstream system while the upstream regulator remains compromised.
For the executive running consequential decisions across three markets, a reduction in mitochondrial ATP efficiency is not an abstraction. It is the biological substrate of slower processing speed, reduced working memory capacity, and diminished stress tolerance. The Philadelphia–Naples–Palm Beach circuit, unmanaged, creates exactly those conditions on a recurring basis.
What Resilient Microbiomes Do Differently
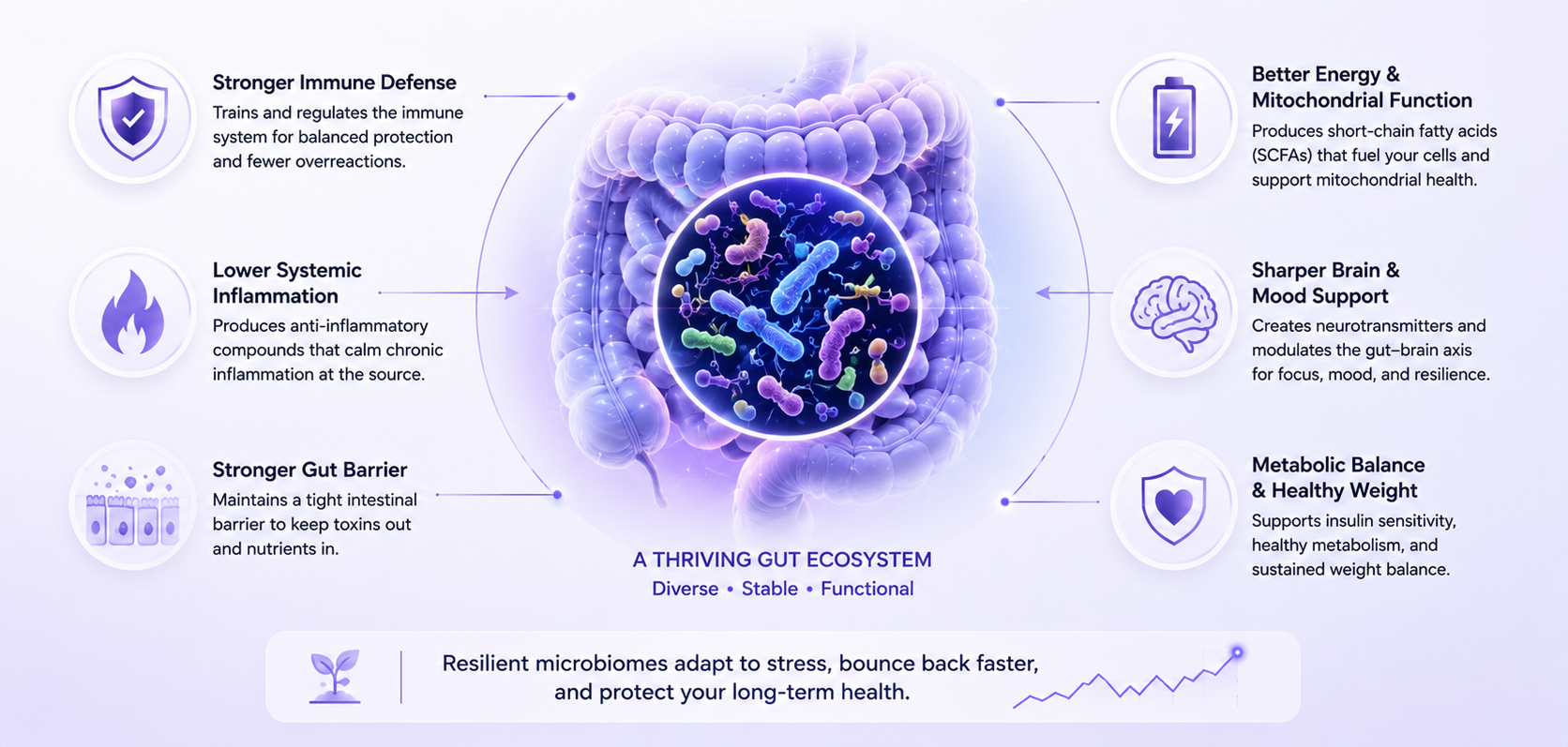
The athletes studied in the Irish cricket cohort—an elite group with high baseline fitness and structured nutritional support—still showed reductions in alpha diversity and shifts in taxonomic profiles following travel. Fitness and general health do not confer microbiome resilience. What does?
Pre-travel microbial diversity is the primary buffer variable. Higher baseline diversity correlates with faster compositional recovery after perturbation events. This is the ecological stability principle applied to the gut: diverse ecosystems absorb disruption more effectively than simplified ones because functional redundancy—multiple species capable of performing the same metabolic tasks—maintains critical outputs (butyrate production, barrier integrity) even as individual species populations fluctuate.
Butyrate-producing taxa, specifically Faecalibacterium prausnitzii, Akkermansia muciniphila, Christensenellaceae, and Ruminococcaceae, are the functional anchors. Their depletion is the earliest measurable signal of travel-induced dysbiosis, and their preservation is the primary objective of any pre- and peri-travel biological resilience strategy.
The Longevity Perspective
The Philadelphia–Naples–Palm Beach circuit is an asset—the ability to operate across three distinct environments is a function of success, not a problem to be solved. The clinical goal is not to eliminate travel but to prevent the cumulative biological cost of recurring unmanaged perturbation from expressing itself years earlier than it otherwise would.
What we are protecting is not gut comfort. We are protecting butyrate production, which sustains intestinal barrier integrity, which governs systemic inflammatory tone, which is upstream of mitochondrial efficiency, cognitive performance, and biological age acceleration. The microbiome is not a peripheral wellness variable—it is the regulator of the biological systems that determine how you age.
If you are making this transition more than four times annually across the Southwest Florida and Palm Beach corridor and have not formally assessed your baseline microbiome composition, inflammatory markers, and gut barrier function, you are managing a consequential biological asset without a dashboard. The diagnostic work is straightforward. The window to intervene early—before the cumulative deficit becomes clinically visible—is finite.
The three-phase clinical protocol for high-frequency travelers across the Philadelphia–Naples–Palm Beach circuit is available as a complete clinical reference document—including pre-departure, in-transit, and stabilization interventions with specific clinical rationale.
Dr. Banerjee is a board-certified gastroenterologist with over 15 years of clinical experience, peer-reviewed publications indexed in PubMed, and deep expertise in gut microbiome science. He advises high-achieving individuals and families on precision longevity and healthspan optimization across Pennsylvania, Florida, and Texas.
Selected References
1. Thaiss CA, Zeevi D, Levy M, et al. Transkingdom control of microbiota diurnal oscillations promotes metabolic homeostasis. Cell. 2014;159(3):514-529.
2. Matenchuk BA, Mandhane PJ, Kozyrskyj AL. Sleep, circadian rhythm, and gut microbiota. Sleep Medicine Reviews. 2020;53:101340.
3. Li Q, Wang B, Qiu HY, et al. Chronic jet lag exacerbates jejunal and colonic microenvironment in mice. Frontiers in Cellular and Infection Microbiology. 2021;11:648175.
4. Olson M, Withrow D, Koelbel M, et al. Sleep and circadian rhythm health on gastrointestinal microbiota. Sleep Medicine Reviews. 2026;86:102256.
5. Bautista J, et al. Bidirectional interactions between circadian rhythms and the gut microbiome. Applied Microbiology and Biotechnology. 2025;109(1):218.
6. DuPont HL. Microbiome alterations during and after international travel. Journal of Travel Medicine. 2025.
7. Worby CJ, Sridhar S, Turbett SE, et al. Gut microbiome perturbation and international travel. The Lancet Microbe. 2023;4(10):e790-e799.
8. Boolchandani M, et al. Impact of international travel and diarrhea on gut microbiome dynamics. Nature Communications. 2022;13(1):7485.
9. O’Donovan CM, et al. Altered gut microbiomes among Irish cricketers over periods of travel. Travel Medicine and Infectious Disease. 2020;35:101553.
10. Cheng M, et al. Microbiome resilience and health implications for people in half-year travel. Frontiers in Immunology. 2022;13:848994.

Should You Get a Gut Microbiome Test? A Gastroenterologist’s Evidence-Based Perspective
Last week, a patient arrived in my clinic with results from a direct-to-consumer gut microbiome test. The report labeled her as “deficient” in multiple bacterial species and recommended several probiotic supplements. It included polished graphics, percentile rankings, and a composite “dysbiosis score.”
The challenge was not the presentation—it was the interpretation. The test measured relative bacterial abundance, not microbial function. The reported “deficiencies” reflected comparisons to a reference population of uncertain clinical relevance, rather than actionable biological deficits. Without functional context, these results risked driving unnecessary interventions and expense.
This scenario is increasingly common. As gut microbiome testing becomes more accessible, patients and clinicians alike are confronted with reports that appear precise but often lack clinical clarity. Understanding what these tests measure, their limitations, and when they add real value is essential.
In this article, I will clarify how gut microbiome tests work, what they can and cannot tell us, and how to determine whether testing is appropriate for your health goals.
Executive Summary
- The gut microbiome plays a central role in metabolism, inflammation, immune regulation, and overall healthspan
- Gut microbiome testing analyzes stool samples using DNA sequencing to assess microbial composition and functional capacity
- The two primary testing methods—16S rRNA sequencing and shotgun metagenomic sequencing—offer different levels of insight and clinical utility
- Microbiome tests do not diagnose disease and represent a snapshot in time, not a fixed biological state
- When interpreted appropriately, microbiome testing can enhance precision care; when used in isolation, it can be misleading

The Core Question: What Are We Actually Measuring?
Modern microbiome tests use DNA sequencing to identify microorganisms in your stool. But not all sequencing methods are created equal, and understanding the difference is critical to interpreting what your results actually mean.
16S rRNA Gene Sequencing: The Industry Standard
This is what most consumer tests and many clinical labs use. It works by targeting a specific bacterial gene—the 16S ribosomal RNA gene—that serves as a genetic fingerprint for bacterial identification.
What it does well:
- Identifies bacteria at the genus level (like identifying "Bifidobacterium" but not which specific species)
- Provides a snapshot of overall microbial diversity
- Relatively affordable and fast
- Uses well-established reference databases
Critical limitations:
- Measures relative abundance, not absolute numbers. If you have less Bacteroides, it might mean you actually have fewer Bacteroides, or it could just mean other bacteria increased. The test can't tell the difference.
- Limited species/strain identification. This matters because Lactobacillus rhamnosus GG has clinical evidence, but "Lactobacillus genus" tells us almost nothing actionable.
- No functional information. It's like having a list of kitchen ingredients but no idea what meal you can make. Knowing bacteria are present doesn't tell you what they're producing.
My clinical perspective: 16S sequencing gives you a compositional overview—useful for assessing severe dysbiosis or tracking major shifts after intervention, but often insufficient for precision treatment planning.
Shotgun Metagenomic Sequencing: The Comprehensive Approach
This method sequences all the DNA in your stool sample—not just bacterial genes, but everything present.
What it offers:
- Species and strain-level identification
- Detection of bacteria, archaea, fungi, and viruses
- Functional profiling—analysis of metabolic pathways and gene capacity
- Insight into antimicrobial resistance genes
Why this matters for longevity: Functional data tells us whether your microbiome has the genetic machinery to produce butyrate, metabolize polyphenols, synthesize certain vitamins, or generate inflammatory compounds. This is clinically meaningful information that composition alone cannot provide.
The trade-offs:
- Higher cost
- More complex interpretation
- Requires sophisticated bioinformatics and clinical integration
- Still doesn't tell us what's actually being produced in real-time
When I order shotgun sequencing: For complex cases with treatment-resistant symptoms, metabolic dysfunction despite dietary optimization, or when I need to understand functional capacity before targeted interventions.
What Microbiome Testing Is Not
Let's clear up common confusion:
Traditional stool tests (culture, ova & parasite exams, PCR panels) are not microbiome tests. These look for specific pathogens—they're diagnostic tools for acute infections, not ecosystem profiling. They won't tell you about diversity, composition, or functional capacity.
Blood tests for "leaky gut" or food sensitivities are not microbiome tests. While gut barrier function and immune responses relate to the microbiome, these tests measure different phenomena and shouldn't be conflated with microbiome analysis.
The Technologies You'll Hear About Next
The field is evolving rapidly. Here's what's emerging from research into clinical practice:
Metatranscriptomics: Instead of DNA, this measures RNA. Think of it as the difference between having a recipe book and actually cooking the meal.
Metabolomics: Directly measures the chemical compounds produced by your microbiome—short-chain fatty acids, bile acids, tryptophan metabolites. This is the closest we get to understanding actual physiological impact, and in my view, represents the future of actionable testing.
Mycobiome and virome analysis: Specialized sequencing for fungal communities and bacteriophages. Emerging evidence suggests these play significant roles in health, but clinical applications are still being defined.
These technologies are mostly research-based today but will likely become standard within 5-10 years as costs decrease and interpretation frameworks mature.
My Clinical Framework
When patients ask about microbiome testing, I walk through these questions to maximize the value of their investment:
- What specific question are we trying to answer? "I want to optimize my gut health" is too vague. "I want to understand why I'm still bloated despite FODMAP elimination" is actionable and guides us toward the right test.
- Will the results guide personalized intervention? Testing shines when it reveals specific imbalances that direct targeted treatment—whether that's particular prebiotic fibers, antimicrobial protocols, or dietary modifications you wouldn't have tried otherwise.
- Are we measuring the right thing? Matching the test to your clinical picture maximizes insight. Functional analysis for metabolic concerns, compositional assessment for dysbiosis, targeted sequencing when specific organisms are suspected.
- How will we integrate results with your complete picture? Microbiome data becomes powerful when combined with your symptoms, dietary patterns, medication history, and inflammatory markers—this integration reveals patterns single data points miss.
- What's the intervention and reassessment plan? The greatest value comes from testing, implementing targeted changes, then retesting to confirm improvement—creating a feedback loop that refines your personalized protocol.
The Bottom Line
Microbiome testing can be a valuable clinical tool when:
- Ordered for specific indications, not general curiosity
- Interpreted by someone who understands both the technology and the clinical context
- Used to guide targeted interventions, not generate anxiety about bacterial "deficiencies"
- Followed by appropriate reassessment to measure intervention success.
The microbiome matters immensely for healthspan and longevity. But understanding what to measure, when to measure it, and how to act on results separates useful clinical data from expensive noise.
Dr. Banerjee is a board-certified gastroenterologist with over 15 years of clinical experience, peer-reviewed publications indexed in PubMed, and deep expertise in gut microbiome science. He advises high-achieving individuals and families on precision longevity and healthspan optimization. Expanded clinical analysis is available through the Private Longevity Briefing.
Selected Peer-reviewed evidence
- Chen S, Chen W, Wang X, Liu S. Mendelian randomization analyses support causal relationships between gut microbiome and longevity. J Transl Med. 2024;22(1):1032. Published 2024 Nov 16. doi:10.1186/s12967-024-05823-2
- Zhang G, Lu Y, Wang Z, et al. Causal relationship between gut microbiota and ageing: A multi-omics Mendelian randomization study. Arch Gerontol Geriatr. 2025;131:105765. doi:10.1016/j.archger.2025.105765
- Liu X, Zou L, Nie C, et al. Mendelian randomization analyses reveal causal relationships between the human microbiome and longevity. Sci Rep. 2023;13(1):5127. Published 2023 Mar 29. doi:10.1038/s41598-023-31115-8
- He D, Liu L, Zhang Z, et al. Association between gut microbiota and longevity: a genetic correlation and mendelian randomization study. BMC Microbiol. 2022;22(1):302. Published 2022 Dec 13. doi:10.1186/s12866-022-02703-x
- Porcari S, Mullish BH, Asnicar F, et al. International consensus statement on microbiome testing in clinical practice. Lancet Gastroenterol Hepatol. 2025;10(2):154-167. doi:10.1016/S2468-1253(24)00311-X

Insulin Resistance Starts in Your Gut—Why Your Glucose Meter Isn’t Telling the Full Story
A 47-year-old executive came to my clinic frustrated. Despite cutting sugar, tracking macros, and exercising six days a week, her fasting glucose crept from 92 to 98 mg/dL over two years. Her physician reassured her she was “fine—not even pre-diabetic yet.”
The problem? She wasn’t fine. Microbiome analysis revealed severely depleted butyrate-producing bacteria and an overgrowth of pro-inflammatory taxa. Her insulin resistance had been developing silently for years—we were just looking in the wrong place.
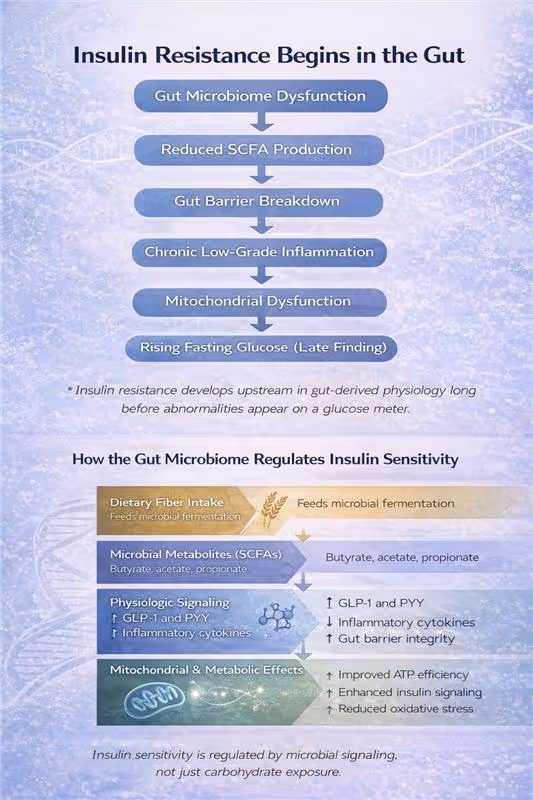
By the time fasting glucose values become abnormal, it’s often too late to catch early dysfunction. Research increasingly shows that insulin resistance begins in the gut, often a decade before traditional blood sugar tests detects it. Understanding this early microbial contribution is key to preventing and reversing metabolic dysfunction.
Executive Summary
- Insulin resistance begins in the gut, often years before glucose becomes abnormal
- Microbial diversity and butyrate-producing bacteria are central to insulin sensitivity
- Short-chain fatty acids act as metabolic regulators, not just digestive byproducts
- Cutting sugar without supporting gut health misses the underlying mechanism
- Early detection through microbiome and insulin assessment enables preventive intervention
- Metabolic resilience—not just lower glucose—should be the goal
Why Your Glucose Meter Tells an Incomplete Story
Insulin sensitivity reflects how efficiently your tissues—muscle, liver, and fat—respond to insulin's signal to take up and use glucose. When sensitivity declines, your pancreas compensates by pumping out more insulin to maintain normal glucose levels.
This means you can have completely normal fasting glucose and HbA1c while your insulin levels are silently climbing—a state called compensatory hyperinsulinemia. This precedes metabolic syndrome and type 2 diabetes by years, sometimes decades.
Here's what most people miss: This early dysfunction doesn't start with excess sugar intake. It begins with gut-derived inflammation, altered microbial metabolite production, and impaired intestinal barrier integrity. Your gut microbiome is an upstream regulator of metabolic health, not a passive bystander.
The Microbiome Signature of Insulin Resistance
Large-scale microbiome analyses consistently show that metabolic health correlates with two key microbial features:
Higher microbial diversity associates with lower insulin resistance and reduced type 2 diabetes risk. A recent JAMA Network Open study identified specific bacterial families—particularly butyrate-producing taxa like Christensenellaceae and Ruminococcaceae—whose presence predicts metabolic resilience.
Microbial composition shifts precede metabolic disease. Before glucose becomes abnormal, insulin-resistant individuals show:
- Depletion of beneficial bacteria (Akkermansia muciniphila, Faecalibacterium prausnitzii, Bifidobacterium species)
- Enrichment of proinflammatory taxa (particularly E. coli and related species)
- Reduced capacity for fiber fermentation and SCFA production
This isn't just correlation. These microbial changes drive the inflammatory and metabolic dysfunction that impairs insulin signaling.
How Your Gut Bacteria Control Glucose Metabolism
The gut microbiome influences insulin sensitivity through multiple interconnected pathways:
Short-Chain Fatty Acid Production
When beneficial bacteria ferment dietary fiber, they produce short-chain fatty acids (SCFAs)—primarily butyrate, acetate, and propionate. These molecules are metabolic regulators, not just byproducts:
- SCFAs stimulate GLP-1 secretion from intestinal cells, enhancing glucose-dependent insulin release and improving postprandial glucose control
- Butyrate activates AMPK signaling in muscle and liver, directly improving insulin sensitivity and metabolic flexibility
- SCFAs strengthen intestinal barrier integrity, reducing endotoxin translocation that triggers systemic inflammation
This positions fiber-fermenting bacteria as functional regulators of your metabolic state. When these bacteria are depleted, SCFA production drops—and insulin sensitivity follows.
Inflammatory Tone and Barrier Function
A compromised intestinal barrier allows bacterial fragments (lipopolysaccharide/LPS) to enter circulation, triggering chronic low-grade inflammation. This "metabolic endotoxemia" impairs insulin receptor signaling in muscle, liver, and fat tissue—creating insulin resistance independent of caloric intake or body weight.
Carbohydrate Processing Efficiency
Multi-omics studies reveal that insulin-resistant individuals have elevated fecal carbohydrates—particularly host-accessible monosaccharides. This indicates inefficient microbial processing: dietary carbohydrates pass through without being converted to beneficial SCFAs.
In contrast, microbiomes with robust fiber-fermenting capacity efficiently convert dietary carbohydrates into metabolic regulators. This is why carbohydrate quality and microbial function matter more than carbohydrate quantity alone.
Gut-Brain and Bile Acid Pathways
Additional mechanisms include gut-brain neuronal signaling that modulates hypothalamic insulin sensitivity and microbial modification of bile acids that influence glucose homeostasis through receptor-mediated pathways. The gut functions as a metabolic command center, not just a digestive tube.
Why Cutting Sugar Isn't Enough
Reducing sugar intake may improve glucose readings short-term, but it doesn't address the biological drivers of insulin resistance. Worse, excessive carbohydrate restriction often reduces dietary fiber intake—inadvertently depleting the butyrate-producing bacteria that protect metabolic health.
I've seen this repeatedly: patients cut carbs to single digits, lose the initial weight, then plateau with persistent inflammation and poor metabolic flexibility. Their microbiome testing reveals the problem: they eliminated fiber along with sugar, collapsing microbial diversity.
The real objective isn't just lower glucose values—it's metabolic resilience: the capacity to manage glucose efficiently across varying dietary, training, and stress conditions. That resilience is built in the gut.
My Clinical Approach
When patients come to me concerned about insulin resistance or early metabolic dysfunction, I start with comprehensive metabolic assessment—looking beyond standard glucose markers to include insulin levels, inflammatory markers, and microbiome function when indicated.
From there, we develop a targeted protocol that addresses the root causes: optimizing fiber intake and microbial diversity, supporting SCFA production, reducing gut-derived inflammation, and implementing lifestyle factors that enhance insulin sensitivity. The specific interventions are personalized based on your unique metabolic profile and microbiome findings.
This systematic approach catches metabolic dysfunction early—before glucose becomes abnormal and tissue damage accumulates.
The Early Detection Advantage
Here's what excites me about this gut-first approach: we can identify and intervene on insulin resistance years before conventional markers flag a problem.
A microbiome depleted in butyrate-producers with elevated inflammatory taxa tells me insulin resistance is developing—even when fasting glucose is 85 mg/dL. This allows for early, targeted intervention when reversal is most achievable.
Compare this to waiting until fasting glucose hits 100 mg/dL or HbA1c reaches 5.7%—at that point, you've already spent years in a pro-inflammatory, insulin-resistant state causing cumulative tissue damage.
The gut microbiome provides a metabolic early-warning system. We just need to listen to it.
The Longevity Perspective
Insulin sensitivity isn't just about avoiding diabetes—it's a central pillar of healthspan. Insulin resistance accelerates aging biology through multiple mechanisms: chronic inflammation, mitochondrial dysfunction, advanced glycation end products, and impaired cellular repair processes.
Maintaining insulin sensitivity as you age requires addressing the biological system that regulates it: your gut microbiome. This means supporting microbial diversity, optimizing fiber fermentation, maintaining barrier integrity, and minimizing inflammatory signals from the gut.
When patients ask me about longevity interventions, metabolic health through microbiome optimization consistently ranks at the top. It's foundational, modifiable, and has cascading benefits across every physiological system.
Dr. Banerjee is a board-certified gastroenterologist with over 15 years of clinical experience, peer-reviewed publications indexed in PubMed, and deep expertise in gut microbiome science. He advises high-achieving individuals and families on precision longevity and healthspan optimization. Expanded clinical analysis is available through the Private Longevity Briefing.
Peer-Reviewed Clinical and Mechanistic Research
- Canfora EE, Meex RCR, Venema K, Blaak EE. Gut microbial metabolites in obesity, NAFLD and T2DM. Nat Rev Endocrinol. 2019;15(5):261-273. doi:10.1038/s41574-019-0156-z
- Cani PD, Amar J, Iglesias MA, et al. Metabolic endotoxemia initiates obesity and insulin resistance. Diabetes. 2007;56(7):1761-1772. doi:10.2337/db06-1491
- Camilleri M. Leaky gut: mechanisms, measurement and clinical implications in humans. Gut. 2019;68(8):1516-1526. doi:10.1136/gutjnl-2019-318427
- Hotamisligil GS. Inflammation and metabolic disorders. Nature. 2006;444(7121):860-867. doi:10.1038/nature05485
- Imdad S, Lim W, Kim JH, Kang C. Intertwined Relationship of Mitochondrial Metabolism, Gut Microbiome and Exercise Potential. Int J Mol Sci. 2022;23(5):2679. Published 2022 Feb 28. doi:10.3390/ijms23052679